Fact Finder - History
Heart-Lung Machine
You might take a beating heart for granted, but surgeons once couldn't touch it without killing the patient. That changed when one determined doctor spent nearly two decades perfecting a machine that could breathe and pump blood for you. It's a story of obsession, failed experiments, and an unlikely partnership with IBM. What that machine made possible — and what it looks like today — will change how you think about modern medicine.
Key Takeaways
- John H. Gibbon Jr. spent 18 years developing the heart-lung machine after watching a patient die from a pulmonary embolism in 1931.
- IBM chairman Thomas Watson funded three successive machine versions over eight years, making the device's development a unique surgical-industrial collaboration.
- The first successful open-heart surgery using the machine was performed May 6, 1953, on 18-year-old Cecelia Bavolek.
- Blood contact with the artificial circuit triggers a systemic inflammatory response involving complement activation, leukocytes, and cytokines.
- Some membrane oxygenators have been reported functioning up to sixteen days, far exceeding the standard six-hour manufacturer recommendation.
How One Surgeon's 20-Year Obsession Produced the First Heart-Lung Machine
In 1931, a patient dying from a massive pulmonary embolism sparked Dr. John H. Gibbon Jr.'s obsession with building a mechanical heart-lung substitute. Witnessing a failed surgical embolectomy with an impossibly high mortality rate, he dedicated the next two decades to solving what conventional medicine deemed impossible.
Gibbon's perseverance drove him to begin formal laboratory work at Massachusetts General Hospital in 1934. His wife, Mary Gibbon, worked alongside him as a true research partner throughout every stage of development. Their early experiments on cats involved rerouting blood through an external oxygenation device, and by 1942, the machine successfully kept cats alive during bypass procedures.
Eighteen years of relentless engineering and animal experimentation ultimately laid the groundwork for the first successful human application in 1953. The critical breakthrough in oxygenator design came when Gibbon's team lined the device's chamber with stainless-steel wire mesh screens, which created turbulence that enhanced gas exchange without destroying blood cells through foaming. The engineering collaboration was made possible after IBM chairman Thomas Watson agreed to fund the full cost of developing three successive machines over eight years.
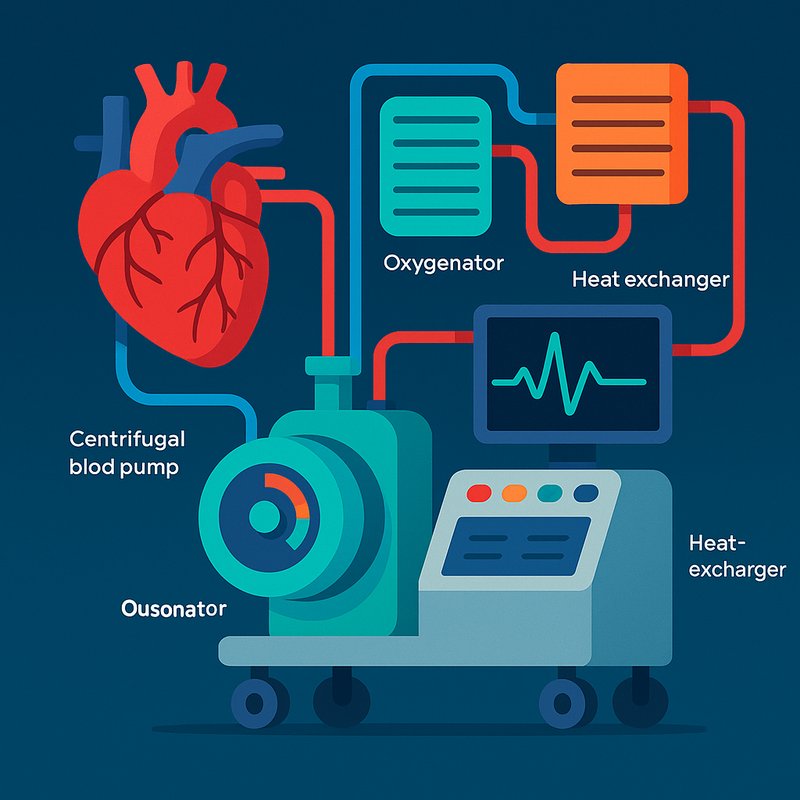
The Pump, Oxygenator, and Heat Exchanger: What Each Component Does
When blood enters the heart-lung machine, three core components work in sequence to keep you alive: the pump, the oxygenator, and the heat exchanger.
Pump mechanics rely on either centrifugal or roller designs. Centrifugal pumps use rotating cones to propel blood through centrifugal force, generating up to 900 mm Hg of forward pressure. Roller pumps peristaltically massage tubing to move blood but carry higher risks of over-pressurization and air embolism.
The oxygenator acts as your artificial lungs, removing carbon dioxide and restoring oxygen. Oxygenator materials include heparin-coated internal surfaces that prevent dangerous clotting throughout the circuit. Manufacturers recommend a maximum use of six hours, though membrane oxygenators have been reported to function for up to sixteen days.
The heat exchanger controls your body temperature, cooling you down to reduce your brain's oxygen demands during surgery. Together, these three components maintain full circulation while your heart stays completely still. Before the circuit is activated, tubing is carefully filled with a priming solution to prevent air embolism and ensure no dangerous air pockets enter the bloodstream.
How the Heart-Lung Machine Keeps You Alive During Surgery
Every parameter gets monitored and adjusted in real time by a certified perfusionist. The machine simultaneously oxygenates the blood and removes carbon dioxide to ensure your organs receive a continuous and adequate oxygen supply throughout the procedure. Contact between blood and the artificial surfaces of the circuit triggers a systemic inflammatory response involving complement activation, leukocytes, and cytokines.
How the Heart-Lung Machine Stops the Heart During an Operation
Stopping the heart during open-heart surgery is a precise, coordinated process that the surgical team executes in careful sequence. Once cannulation establishes full bypass support, they cool your blood through the heart-lung machine's heat exchanger, reducing your heart's oxygen demand before arrest.
Cardioplegia timing matters here — the team applies the aortic cross-clamp first, blocking coronary blood flow, then injects a potassium-rich cardioplegia solution through your coronary arteries. This halts your heart's electrical activity, producing diastolic arrest.
Venous isolation follows, clamping your venous line to prevent blood from returning to the now-still heart. The result is a motionless, bloodless surgical field. Your surgeon can then operate precisely while the heart-lung machine sustains your circulation and oxygenation throughout. Once the procedure is complete, the team restarts your heart by flushing out the cardioplegia solution, administering a reversing agent, or delivering a mild electric shock.
The heart-lung machine is operated by perfusion technologists, specialized members of the surgical team who manage the equipment and can sustain your circulation in this capacity for several hours. Advances in standardized medical training have helped ensure that perfusion technologists and supporting staff are consistently prepared to operate this critical equipment across a wide range of hospital settings.
The Surgeries That Were Impossible Before the Heart-Lung Machine
Before the heart-lung machine existed, surgeons couldn't access the heart's interior without killing the patient. Congenital repairs and valve accessibility were impossible since blood flow obscured the surgical field completely.
Here's what the machine finally made possible:
- Atrial septal defect closure — Gibbon repaired Cecelia Bavolek's heart hole successfully in 1953
- Aortic reconstruction — combined cooling below 28℃ enabled complex narrowing corrections
- Congenital repairs — Mayo Clinic performed eight successful open-heart surgeries in 1955
- Valve accessibility — surgeons could suture interior structures without active blood flow interfering
- Reliable survival rates — early bypass cases replaced the previous 17 deaths in 18 attempts
These breakthroughs transformed cardiac surgery worldwide. The device also became essential support for heart transplant patients, who relied on maintained circulation and oxygenation throughout the procedure. John Gibbon's research began after a patient's death during cardiac surgery in 1931 inspired him to develop an external device capable of maintaining blood circulation artificially.
How Portable Heart-Lung Machines Changed Emergency Care
Traditional heart-lung machines have always been anchored to the operating room, but portable ECMO systems have broken that barrier entirely. You can now deploy mobile ECMO directly at a patient's bedside, inside ambulances, or even aboard ships and planes. Systems like the MOBYBOX fit into a backpack, while the Breethe OXY-1 starts up in under two minutes, making prehospital resuscitation a realistic option for cardiac arrest and cardiogenic shock victims.
These advancements translate directly into saved lives. In one Massachusetts case, a portable lung bypass machine reached a mother before traditional transport was possible. Among patients with severe hemodynamic compromise without full cardiac arrest, three out of three achieved long-term survival, demonstrating that early, mobile intervention dramatically improves outcomes when every second counts. However, research highlights a stark contrast for full cardiac arrest patients, where overall survival rates using portable cardiopulmonary bypass remain critically low at just 3.4 percent.
The Breethe OXY-1 also represents a landmark shift in patient comfort and recovery, as the device was used at the University of Maryland Medical Center to allow patients to ambulate during oxygenation, reducing breathlessness and improving mobility compared to traditional ECMO setups.
Why the Heart-Lung Machine Revolutionized Open-Heart Surgery
When the heart-lung machine entered operating rooms in 1953, it didn't just improve cardiac surgery — it made it possible. By maintaining circulation artificially, surgeons gained the surgical precision needed to work directly inside the heart, transforming patient outcomes permanently.
Here's what that revolution delivered:
- First successful open-heart surgery performed May 6, 1953, on 18-year-old Cecelia Bavolek
- Extended operative time allowed complex repairs impossible under natural circulation
- Tetralogy of Fallot mortality dropped from 50 percent in 1955 to near zero by 1980
- Heart transplants became achievable, beginning December 3, 1967
- Nearly 70 percent of open-heart surgery patients now resume full lifestyles
Every modern cardiac procedure traces its foundation directly back to this single technological breakthrough. The device itself was the result of 18 years of experimental engineering and animal work carried out by John H. Gibbon Jr. before it was ever used on a human patient. John Kirklin's modified version of the machine, developed at Mayo Clinic, proved its safety when nine of 10 dogs survived up to 60 minutes on the device without discernible ill effects during animal testing.