Fact Finder - Science and Nature
Flexibility of the Ear: The Eustachian Tube
The Eustachian tube is a narrow canal connecting your middle ear to the back of your throat, and it handles more than you'd expect. It equalizes pressure, drains fluid, and blocks harmful bacteria — all while staying closed most of the time. It only opens for about 0.4 seconds when you swallow or yawn. Stick around, because there's a lot more fascinating detail about how this tiny tube keeps your ears working.
Key Takeaways
- The Eustachian tube has two distinct sections: a rigid 12mm bony section and a flexible 24mm cartilaginous section.
- The tube stays closed most of the time, briefly opening for just 0.4 seconds during swallowing, yawning, or chewing.
- Multiple muscles, including the tensor veli palatini, work together to dynamically pull the tube open when needed.
- The tube's flexible cartilaginous section allows it to respond to jaw and throat movements for pressure regulation.
- In infants, the tube sits at a more horizontal angle, making it more flexible to bacterial transfer from the nose.
What Is the Eustachian Tube and What Does It Do?
The Eustachian tube — also called the auditory or pharyngotympanic tube — is a narrow osseo-fibrocartilaginous canal that connects your middle ear to the nasopharynx. It extends from the bony portion in your temporal bone to the lateral fibrocartilaginous wall of the nasopharynx, remaining closed most of the time.
This tube performs several critical functions. It drains fluid, equalizes air pressure, and oxygenates your tympanic cavity — all essential for healthy middle ear biomechanics. It also shields your middle ear from pathogens present in the nasopharyngeal microbiome, acting as a barrier against harmful viruses and bacteria.
The tube opens during swallowing, yawning, and chewing, allowing small amounts of air to enter and maintain proper pressure balance across your eardrum. The tube itself is named for Bartolomeo Eustachi, the anatomist credited with discovering its connection between the middle ear and throat.
Why the Eustachian Tube Is Built in Two Different Sections
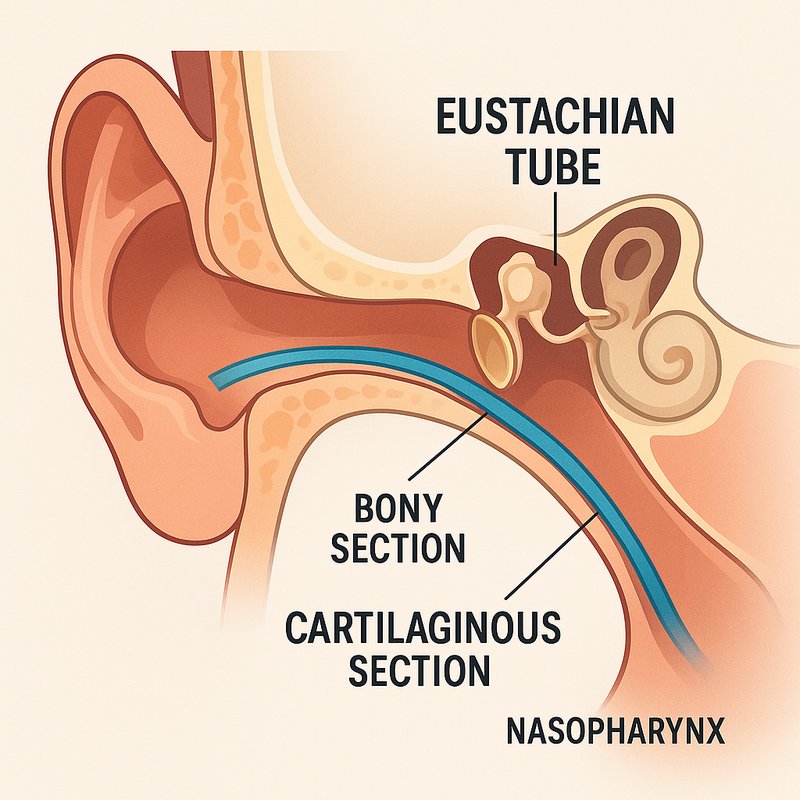
Unlike most tubular structures in the body, the Eustachian tube isn't built from a single uniform material — it's constructed in two distinct sections that differ in composition, length, and mechanical role.
The shorter bony section, roughly 12mm, sits anchored within the temporal bone and handles rigid pressure resistance.
The longer cartilaginous section, approximately 24mm, sits within soft tissue and flexes during pressure equalization through muscular action.
Their separate developmental origins explain why each section carries its own vascular supply, tissue properties, and structural behavior.
Where the two sections meet, the isthmus forms the tube's narrowest point, controlling airflow direction.
Understanding this two-part design matters considerably for surgical considerations, since interventions affecting one section don't necessarily behave the same way in the other. The osseous portion's roof contains a dedicated canal housing the tensor tympani muscle, which plays a primary role in the acoustic reflex alongside a secondary role in tube opening.
Which Muscles Control the Eustachian Tube?
Knowing how the Eustachian tube's two-section structure works sets up a logical question: what actually moves it?
Six muscles control Eustachian tube function through coordinated palatal mechanics and precise muscle innervation:
- Tensor veli palatini – the primary opener, pulling the tube's lateral wall outward during swallowing and yawning, driven by trigeminal nerve V3
- Levator veli palatini – a secondary contributor that elevates your soft palate while assisting cartilaginous opening, controlled by the vagus nerve
- Tensor tympani, salpingopharyngeus, lateral pterygoid, and medial pterygoid – supporting players that enable peristaltic tube movement and pressure regulation
Your mandible and pharynx movements trigger these contractions automatically. Without this muscular teamwork, your tube would stay permanently closed, leaving you unable to equalize ear pressure. The tensor tympani, for instance, originates from the cartilaginous tube and inserts on the handle of the malleus, where it functions to dampen loud sounds such as those produced during chewing.
What Triggers the Eustachian Tube to Open?
Several automatic triggers open your Eustachian tube without conscious effort. Swallowing activates the tensor veli palatini and levator veli palatini muscles approximately 1.4 times per minute, maintaining routine pressure equalization throughout your day.
Chewing creates similar results, as mandibular movement engages the tensor muscle of the soft palate, triggering intermittent tube dilation. Chewing gum extends this effect through continuous jaw movement, making it a practical pressure-relief strategy.
Altitude yawning delivers a more exaggerated opening motion than swallowing, producing that familiar "popping" sensation as your middle ear pressure equalizes with the atmosphere. When these passive triggers aren't enough during rapid altitude changes or diving, the Valsalva maneuver allows you to consciously force the tube open, complementing your body's natural mechanisms. Each opening event lasts only approximately 0.4 seconds, after which the tube returns to its resting closed position until the next trigger occurs.
How the Eustachian Tube Equalizes Pressure in Your Ear
Your Eustachian tube stays closed most of the time, cracking open only for a fraction of a second during swallowing, yawning, or chewing to let small amounts of air into your middle ear.
For barotrauma prevention during plane acoustics and pressure shifts, your ear handles equalization in three key stages:
- During ascent, positive middle ear pressure pushes your eardrum outward until the tube opens, releasing excess pressure.
- At approximately every 500–1,000 feet, pressure equalizes automatically through brief tube openings.
- During descent, increasing cabin pressure creates negative middle ear pressure, pulling your eardrum inward and making equalization harder.
When equalization fails, trapped air absorbs into surrounding tissue, creating a vacuum effect that causes pain and potential eardrum damage. Colds and ear infections can cause swelling around the Eustachian tube membranes, making it significantly harder to equalize pressure and increasing the risk of middle ear pain.
How Eustachian Tube Pressure Changes Affect Sound Transmission
When pressure in your middle ear falls out of balance, it pulls your eardrum inward, stiffening it and preventing it from vibrating freely. This tension disrupts middle ear resonance, making sounds seem muffled, as if you're underwater or your ears are packed with cotton wool.
As negative pressure accumulates, fluid gets drawn into your middle ear space, creating a physical barrier that interferes with cochlear mechanics by blocking the tiny ear bones from moving properly. Sound waves can't transfer efficiently through this fluid-filled environment, causing conductive hearing loss.
If the dysfunction continues, that trapped fluid can also invite bacterial infections, inflame your middle ear lining, and stiffen the ossicles further, progressively compounding your hearing impairment with each passing day. Left untreated, this progression can lead to permanent eardrum damage, tinnitus, or lasting hearing loss that may require surgical intervention to address.
How the Eustachian Tube Drains Fluid and Prevents Infection
Beyond simply equalizing pressure, your Eustachian tube actively drains fluid from your middle ear, shuttling mucus down toward your nasopharynx where you swallow it away. Its anteroinferior portion drives mucociliary dynamics, using tiny cilia and surfactants to move secretions efficiently.
Three key mechanisms protect your middle ear:
- Mucociliary clearance sweeps bacteria-laden mucus away before pathogens establish themselves
- Immune barriers block rhinopharyngeal microorganisms from traveling backward into your sterile middle ear
- Gravity-assisted drainage improves markedly after age six, as your tube angles more obliquely
When blockage occurs, trapped fluid creates a bacterial breeding ground. Swelling from allergies or infections closes the tube, stalling drainage and triggering the conditions that develop into painful ear infections. In infants and young children, the horizontal tube orientation allows bacteria to transfer more easily from the nose into the middle ear, significantly raising their infection risk.
What Happens When the Eustachian Tube Fails?
The Eustachian tube's failure to regulate pressure and drain fluid sets off a cascade of symptoms that can range from mildly annoying to seriously debilitating. You'll likely notice muffled hearing first, as though you're underwater, followed by a fullness or pressure sensation in your ear. Popping and crackling sounds develop as the tube struggles to open and equalize pressure.
Vestibular symptoms, including dizziness, vertigo, and unsteadiness, emerge when pressure changes and fluid buildup disrupt your inner ear's balance functions. Chronic blockage lasting beyond three months markedly raises your risk of permanent hearing damage. Negative pressure also causes your eardrum to pull inward, intensifying pain as it stretches. Eustachian tube dysfunction is also recognized as a leading cause of otitis media, making recurring ear infections a common consequence of prolonged dysfunction. If symptoms persist beyond one to two weeks, seeking medical attention becomes essential.