Fact Finder - Science and Nature
Smallest Bone: The Stapes
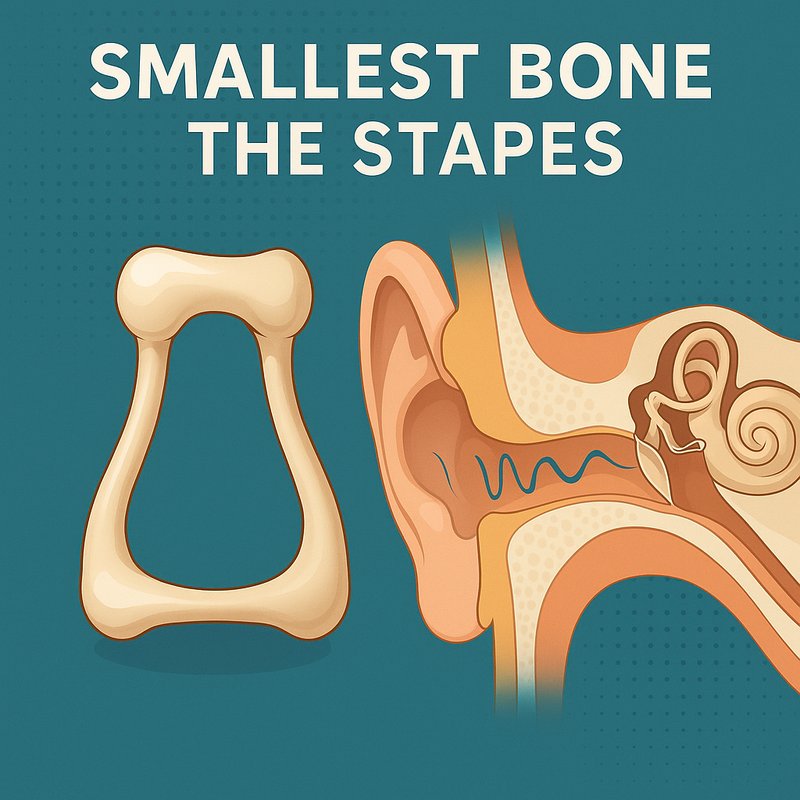
The stapes is the smallest and lightest bone in your body, measuring just 2–3 mm and sitting deep inside your middle ear. It's shaped like a tiny stirrup and plays an essential role in your hearing by transmitting sound vibrations into your inner ear's fluid. It develops from your second pharyngeal arch and completes ossification before you're even born. There's much more to this fascinating little bone than you'd expect.
Key Takeaways
- The stapes, shaped like a tiny stirrup, measures only 2–3 mm and is the smallest and lightest bone in the human body.
- Located in the middle ear, the stapes transmits sound vibrations into cochlear fluid, enabling the conversion of sound into electrical signals.
- The stapes develops from the second pharyngeal arch, with ossification completing by approximately 26 weeks of gestation.
- Otosclerosis can abnormally fix the stapes, causing gradual conductive hearing loss that typically affects low-pitched sounds first.
- The stapes shows greater anatomical variability than any other ossicle, with congenital abnormalities often associated with known syndromes.
What Exactly Is the Stapes Bone?
The stapes is the smallest and lightest bone in the human body, sitting deep within the middle ear cavity inside the temporal bone's petrous part. It's the third and innermost bone of the ossicular chain, following the malleus and incus. Understanding ossicle evolution helps you appreciate why this tiny bone carries such significant responsibility in hearing.
Shaped like a stirrup or horseshoe, the stapes consists of a head, neck, anterior and posterior crura, and a flat footplate at its base. Its head connects to the incus through the incudostapedial joint, while its footplate attaches to the oval window via the annular ligament. Measuring just 2 to 3 mm in length, its minimal mass enables rapid vibratory response to incoming sound stimuli. Pathological conditions such as otosclerosis can affect the stapes, sometimes requiring surgical intervention to restore hearing function.
Why the Stapes Is the Smallest Bone in the Human Body
While the stapes' tiny size might seem incidental, it's actually the product of precise embryological programming. Between weeks six and eight, your stapes develops from the second pharyngeal arch, with the stapedial artery carving out its hollow, stirrup-shaped cavity before regressing. This process locks in its 2-3mm length by design.
Every structural choice reflects biomechanical scaling principles. Its horseshoe configuration provides stability without unnecessary bulk, while its minimal mass reduces inertial resistance, allowing rapid vibration response across audible frequencies. The flat base seals the oval window efficiently, and the small neck supports the stapedius muscle attachment without excess material.
This represents a clear evolutionary advantage: consistent sizing across all human populations confirms that natural selection stabilized these dimensions at their functional optimum for maximum hearing efficiency. The stapes is connected to the incus through the incudostapedial joint, forming a critical link in the ossicular chain that transmits sound to the inner ear.
The Head, Footplate, and Crura: Inside the Stapes' Structure
Nestled within your middle ear, the stapes packs a complete mechanical system into just 2-3mm. Its head, called the capitulum, connects to the incus through a synovial joint complete with a meniscus and fluid capsule. Below the head, the neck branches into two crura—anterior and posterior arches—that distribute vibrational forces down to the footplate.
The footplate anchors into the oval window via an annular ligament, transmitting sound vibrations directly into your cochlear fluid. This stirrup-shaped superstructure functions as one unified mechanical unit, converting incoming sound into fluid motion.
Because the stapes shows the greatest anatomical variability among ossicles, microfracture detection becomes critical during evaluation. Developmental irregularities like crural fusion or thinning directly affect surgical access and influence how effectively your ear conducts sound. The stapes begins ossification around 18 weeks of fetal development, completing the process by approximately 26 weeks gestation.
How the Stapes Transmits Sound to Your Inner Ear
Sound travels a precise mechanical pathway before you ever consciously hear anything. Vibrations enter your ear canal, strike your eardrum, then pass sequentially through the malleus and incus before reaching the stapes. The incus acts as a lever arm, amplifying force before transferring it to your stapes.
Your stapes doesn't move identically across all frequencies. At lower frequencies, it performs a piston-like motion, while higher frequencies trigger rocking movements around its axes. This mechanical variation supports frequency tuning within your auditory system.
The stapes footplate then pushes against your oval window, initiating fluid coupling as energy enters your cochlea. That fluid displacement stimulates hair cells, which convert mechanical motion into electrical signals your brain interprets as sound. Damage to the stapes from conditions like otosclerosis can disrupt this process, leading to conductive hearing loss.
How the Stapes Differs From the Malleus and Incus
Compared to the malleus and incus, the stapes is a genuinely distinct bone in nearly every measurable way. Its differences affect ossicular biomechanics, embryological origin, and clinical imaging visibility.
Key distinctions include:
- Origin: The stapes develops from the 2nd pharyngeal arch, while the malleus and incus derive from the 1st pharyngeal arch.
- Position: The stapes sits deepest in the middle ear, making it the hardest to visualize during clinical imaging and otoscopic examination.
- Variability: The stapes exhibits the greatest anatomical variability among the three ossicles, including aplasia, hypoplasia, and crural fusion.
You'll also find that the stapes articulates with the incus through a synovial joint, whereas the malleus and incus share a saddle joint with different mechanical properties.
All three ossicles are located in the posterior superior section of the tympanic membrane, yet the stapes remains the least accessible of the group due to its depth within the middle ear space.
What Happens When the Stapes Stops Working?
Understanding how the stapes differs from its neighboring ossicles makes its functional role clearer — and when that function breaks down, the consequences are significant.
When abnormal bone growth fuses the stapes in place, it can no longer vibrate freely, blocking sound transmission to your inner ear. This causes conductive hearing loss, with hearing deterioration progressing gradually over years. You'll likely notice difficulty hearing low-pitched sounds first, and the condition often affects both ears eventually.
Beyond hearing, you may also experience balance symptoms if the abnormal bone spreads to your balance canals, causing vertigo and dizziness.
Treatment options include hearing aids, stapedectomy surgery, or cochlear implants in advanced cases. Without intervention, the hearing loss continues worsening, though complete hearing loss remains uncommon. Otosclerosis is the most common cause of middle ear mechanical hearing loss among young adults.
Rare Stapes Conditions and Congenital Variations
While most stapes problems stem from acquired conditions like otosclerosis, some people are born with structural abnormalities that affect how the bone forms or functions. Congenital stapes malformations, including stapes agenesis, follow predictable developmental patterns based on disruptions to mesodermal and neural crest-origin subunits.
Key congenital variations include:
- Stapes fixation – the oval window fails to form properly, sometimes linked to X-linked or NOG-related genetic mutations
- Superstructure misplacement – the stapes separates from its footplate and attaches incorrectly to the promontory
- Absent footplate – the oval window forms but remains covered by a mucosal membrane
Syndromic associations are significant—72% of affected patients carry a known syndrome, including Nager and Otopalatodigital syndromes, complicating both diagnosis and surgical planning.