Fact Finder - Science and Nature
Strength of the Human Femur
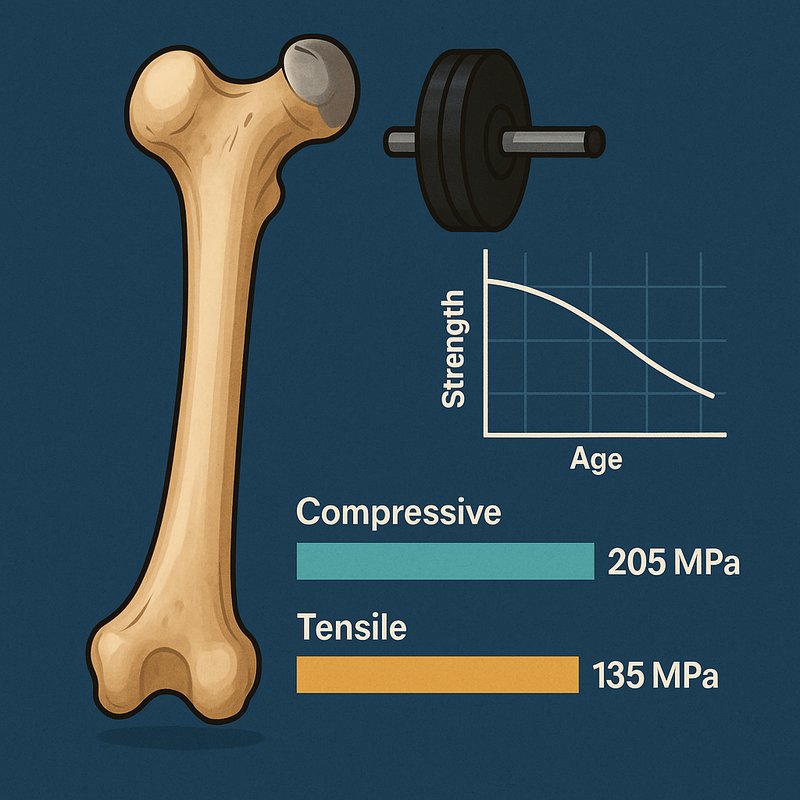
Your femur is the strongest bone in your body, capable of withstanding forces up to 30 times your body weight. It handles more compression than tension, tolerating around 205 MPa compressively versus 135 MPa in tension. Peak strength hits before age 30, after which gradual decline begins — accelerating faster than bone density loss alone would suggest. If you're curious about what's really driving these numbers, there's much more to uncover.
Key Takeaways
- The femur is the body's strongest bone, capable of supporting approximately 30 times a person's body weight under load.
- Compressive strength significantly exceeds tensile strength, with cortical bone withstanding roughly 205 MPa in compression versus 135 MPa in tension.
- Peak femoral strength occurs at age 30 or below, after which both tensile and compressive strength progressively decline with age.
- Men consistently demonstrate higher femoral strength than women, with women experiencing roughly 55% total strength loss by age 85.
- Femoral strength declines more than 40% faster than bone mineral density, making standard screening methods potentially inadequate for fracture risk.
How Strong Is the Human Femur, Really?
The human femur is the strongest bone in the body, capable of supporting roughly 30 times your body weight. This remarkable capacity reflects millions of years of evolutionary adaptation to bipedal locomotion and high-impact physical demands.
Through biomechanical modeling, researchers have confirmed that compressive strength consistently exceeds tensile strength in both men and women. Your femur's peak mechanical performance occurs at age 30 and below, where tensile strength reaches its highest recorded values. Curiously, Young's modulus is lowest in this younger age group, meaning your bone is actually more ductile, not simply harder.
Both tensile and compressive strength decline progressively with age, and male specimens consistently demonstrate higher failure strength across all age groups compared to female specimens. Despite its extraordinary strength, the femur remains vulnerable to high-impact fractures, which typically require significant force such as that generated in car accidents or severe falls.
The Size, Density, and Structure Behind Femur Strength
Measuring in at roughly 48 cm long and 2.34 cm in diameter, your femur isn't just the longest bone in your body — it's also the thickest, sharing the distinction of being among the two strongest bones alongside the temporal bone of the skull. Its bone composition includes cortical bone capable of withstanding 205 MPa of compressive force and 135 MPa of tensile force.
Men's femurs consistently outperform women's, showing an approximately 1,750 N strength advantage that size differences alone don't fully explain. Microarchitecture variation at the tissue level — not just density — drives much of this difference. Bone mineral density in males also exceeds female measurements across all ages, reinforcing why gender and structure both matter when evaluating femoral strength. Because bone exhibits anisotropy, its compressive strength along the longitudinal axis measures notably higher than its transverse compressive strength, which drops to approximately 131 MPa — roughly 36% less.
How the Femur Responds to Compression, Tension, and Microfracture
Bone density and structure tell only part of the story — how your femur actually responds when forces act on it reveals the full picture of its mechanical behavior. Your femur exhibits bone anisotropy, meaning it handles compression far better than tension. Its ultimate compressive strength reaches approximately 205 MPa, while tensile strength measures only around 135 MPa.
Collagen fibrils drive this asymmetry — they're exceptionally strong under tension yet weak under compression. Under repetitive loading, microdamage accumulation becomes your femur's silent threat. Microcracks spread throughout bone tissue during everyday activities, and as they progress, cohesion between microfibrils increases paradoxically, reducing flexibility and crack resistance.
Older bone faces greater risk because reduced collagen fibril diameter and increased fibril stiffness lower resistance to crack propagation. The femur's midshaft cross-section is roughly circular and somewhat hollow, with bone marrow occupying the central cavity, a structural arrangement that optimizes resistance to compressive and tensile forces acting along its length.
How Age and Gender Affect Femur Strength Over Time
Although your femur reaches peak strength around age 30, it doesn't hold that strength equally across genders or through time. Women begin losing femoral strength in their mid-40s, roughly a decade earlier than men, and that earlier onset accounts for about 60% of the strength gap between genders by age 85.
Hormonal changes accelerate cortical bone thinning and proximal femur expansion faster in women than in men. By age 85, women experience approximately 55% total strength loss compared to 39% in men, creating roughly a 1,000 N deficit between the sexes.
Lifestyle factors compound these losses, since strength declines more than 40% faster than bone mineral density in both sexes, making low femoral strength far more prevalent than standard osteoporosis diagnoses suggest. Research using data from over 5,600 adults confirms that men consistently show higher femur neck bone density than women across all measured skeletal sites.
Why Low Femur Strength Makes Fractures Far More Likely
When femoral strength drops below critical thresholds, fracture risk doesn't rise gradually—it spikes dramatically. Every man with femoral strength below 2900 N in prospective studies experienced a hip fracture. That's not a statistical trend—it's a biomechanical threshold with life-altering consequences.
What makes this worse are the diagnostic gaps in current screening. Over half of people who fractured with low femoral strength weren't even classified as osteoporotic—they had osteopenia, a less severe designation that often triggers no intervention. Standard bone density scans simply miss too many high-risk individuals.
Your fracture risk also compounds after an initial break, with 40–60% of survivors experiencing secondary fractures within a decade. Low femoral strength doesn't just increase danger once—it resets your baseline to a permanently higher risk level.